In This Blog, You Will Get To Know:
- What does a clinic look like at 1, 3, 5, or 10+ sites?
- When must a clinic chain build a formal reporting structure?
- How does oversight change as your chain crosses 10 sites?
Good multi-location clinic operations need a clear plan. The structure must change before the cracks show. Clinic chain scaling operations differ at every stage. Each stage needs its own workflow and reporting model.
Stage 1: The Single-Clinic Operational Foundation
What the Workflow Looks Like at One Location
At Stage 1, every task moves along a single line. The flow is simple:
Patient Intake → Scheduling → Provider Assignment → Billing → End-of-Day Check → Owner Review
The owner takes care of all the steps. But that is by design. One sees all: Thus, decision-making is quick. Nothing needs sign-off. There is no more that the founders could not see.
The Governance Reality at Stage 1
Stage 1 is flat. The system is the founder. SOP Formalization Status: Informal, owner-driven actions. They are effective because one person staffs them.
But this is where the base of clinic management software is most crucial. Stage 1 Digital workflows help you avoid broken workflows later. You instead create your own standard for the whole chain to follow.
Stage 3: Building the First Cross-Location Operating System
How Workflows Change Across Three Sites
Three sites make all the difference. The shifting of clinic chain scaling operations here. In multi-site clinic workflow management, there are clear hand-off points now:
Site Intake → Location Manager Huddle → Central Desk → Shared Billing Team → Weekly Sync → COO Review
The steps are executed at different sites. But in fact, the central desk call is the most important one here. If you’re not, your digital patient experience clinic standard erodes quickly.
The starting point for standardizing clinical workflows across different locations. The big change is at Location 3. That’s where the informal systems fail. For instance, the rate of “conflict” increases by 40% for Site 3. This is when no central desk controls are placed across-site slots. Without a central system, there is a cross-location reporting lag of 3-5 business days.
The Clinic Chain Reporting Structure at Three Locations
But workflow is not sufficient. It should be the same as the cross-location clinical reporting. Below is the clinic chain reporting structure for Stage 3:
| ROLE | REPORTS TO | DECISION SCOPE |
| Site Lead (×3) | Ops Manager | Daily scheduling + site staff |
| Ops Manager | Founder / COO | Cross-site workflow + vendors |
| Billing Lead | Ops Manager | Claims + collections, all sites |
| Founder / COO | Board / Self | Strategy + finances |
For instance, if the company is exporting its products to the global markets, the chains need to identify the best clinic management software at an early stage. This model is performed by this selection.
 PRO TIP
PRO TIP
Stage 5: Formalizing the Management Layer
The Clinic Chain Organizational Structure at Five Locations
Five locations have actual risk. The transition in clinic chain scaling needs to be made here. The organizational structure of clinic chains of growth stages has changed now. So the staffing model needs to as well:
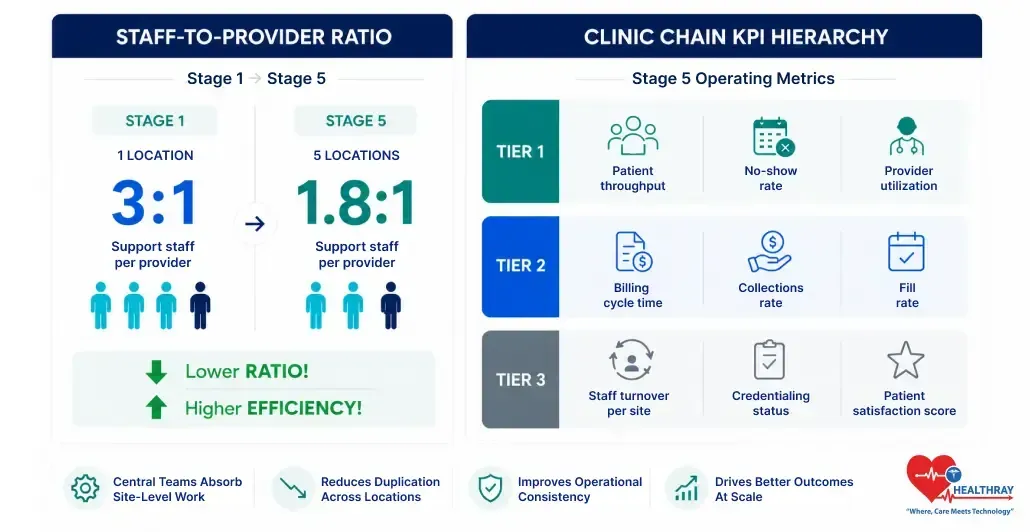
Staff-to-Provider Ratio: 3:1 at Stage 1. It drops to 1.8:1 at Stage 5.
Why? Central teams perform tasks that previously were done at each site. However, those groups that forgo this step ultimately pay the price. This is because groups with no formal layer have higher admin costs based on MGMA benchmarking data. So the gap shows up in the numbers.
But it’s not all about the price. Clinic chain KPIs need to be formalized here:
- Tier 1 KPIs: Patient throughput, no-show rate, provider utilization
- Tier 2 KPIs: Billing cycle time, collections rate, fill rate
- Tier 3 KPIs: Staff turnover per site, credentialing status, patient scores
What Healthcare COO Responsibilities Look Like at Five Locations
Clinic chain organizational structure is based on clear decision rights. But it has to have established meeting cycles also. Stage 5 is characterized by three key meetings. A weekly ops review is the first step. Secondly, a finance meeting once a month. Thirdly, a quarterly clinical audit.
There is an agenda for each meeting. Both have predetermined lists. So that nothing is decided on the spur of the moment.
Workflow automation for doctors lends support to this. Task routing is handled by Auto alerts. That includes that the system operates without additional staff.
 NOTE
NOTE
Stage 10+: Running an Enterprise Clinic Chain
Enterprise Workflow at 10+ Locations
When scaling up healthcare operations at 10+ sites, two layers of ops are created. But every layer is assigned a particular task:
Regional Director → Area Ops Manager → Site Medical Director → Site Lead → Central HQ (Finance | HR | IT | Legal)
The most significant new addition is the Regional Director. If not, the COO has too many direct reports. Each Regional Director gets 4-6 sites. They have control over KPI results, staffing and SOP adherence.
All data across sites is managed by Central HQ. This includes location data on all live sites. In fact, the chain operates on calls in the center and on-site execution. Likewise, construction web design companies are modular, units work as a part of a system.
Healthcare that adheres to role-based access control is the norm in 10+ sites. It regulates access to data and its roles. Here, clinic chain EHR integration plays a pivotal role. No longer a call for the site.
The Healthcare Operational Governance Model at Enterprise Scale
But it’s not the whole thing. In the full clinic chain scaling operations governance model, there are five functions:
| FUNCTION | OWNER | HOW OFTEN | STANDARD |
| ePHI Access Control | IT Director | Live audit log | HIPAA 45 CFR Section 164.312 |
| Clinical Quality Check | Site Medical Director | Each month | Internal QA |
| Finance Review | Central Finance Lead | Each week | Board reporting |
| Staff Credentialing | Central HR Team | 90-day rolling | Payer rules |
| Regional KPI Review | Regional Director | Every two weeks | COO framework |
According to CMS medical records documentation rules, chains of clinics should maintain records at all open locations. That is a standard that the old site-level systems can’t keep up. In truth, the gap isn’t an ops problem, but a compliance risk.
Learn more: At some point, every growing clinic chain faces a build-or-buy decision. When to Build vs Buy Custom Clinic Software Development breaks down exactly how to think through it.
To Sum Up
Clinics that are part of a chain scale up operations in a predictable manner.Clinics within a chain scale predictably. Stage 1 is the founder control stage. For stage 3, a central system is necessary. However, a formal layer with defined oversight is needed for Stage 5. Stage 10+ runs on regional command and enterprise systems.
The structure is clearly defined for each stage. Therefore, make a solid clinic chain growth plan in advance before the current stage breaks.