In This Blog
Everything a clinic manager requires to improve the patient experience digitally before losing patients:
- The five specific operational points that patients disconnect on within your clinic’s digital experience
- Why paper to digital conversion fails without having the right technology layer implemented at each point
- The solution required by the specific infrastructure at each touchpoint – not broad recommendations
- What the data really tells us about patient actions at each and every point
- Completing the loop for creating a comprehensive integrated patient engagement system
Here is something most clinic managers don’t hear until it’s too late: your patients are not leaving because of poor clinical care. They are leaving because of friction – the broken scheduling page, the PDF intake form that won’t open on a phone, the telehealth room link that never arrived.
A genuine digital patient experience clinic framework means every step of the patient journey – from the first Google search to the post-visit follow-up – runs automatically. Clinics that close these gaps report measurably fewer no-shows – studies on digital scheduling and automated reminders consistently show no-show rate reductions of 20–30% – along with faster payment cycles and front-desk staff freed from callback queues. Not a website. Not a patient portal sitting idle. A connected system that moves patients through without making them do the administrative work your software should handle.
This manual is based on the “Five-Touchpoint Digital Model,” which represents five key operational moments where patients experience friction. A well-integrated clinic management software acts as the central system that connects scheduling, intake, billing, and follow-ups, ensuring no patient falls through the cracks. The guide also highlights the exact points where patients drop off during their journey and how clinics can effectively bring them back into the system.
Touchpoint 1 – Online Scheduling Drop-Off: Patients Leaving Before Booking
Friction Point: Your “Book Now” button leads to a static contact form, your phone number, or your clinic hours. The patient is there to make an appointment but must wait rather than book.
A patient is looking for your specialty, finds your listing, clicks through only to encounter a dead end. There is no live calendar with appointments. There is only an appointment form stating someone will get back in touch within 24 hours. The booking decision itself takes less than 90 seconds. The patient moves on to the next search result, and your practice never realizes they were lost.
In a digital patient experience clinic, patients go through five to seven touchpoints before scheduling an appointment with a healthcare provider. Every one of these touchpoints is a point of decision-making. The lack of a live schedule is not just an inconvenience – it is a deal breaker for a patient who has already checked two other providers’ schedules.
Software Fix: Your scheduling API should be integrated directly with your EHR integration layer so that it shows live availability on your website without any intermediary action from your staff. This enables workflow automation for doctors, reducing manual appointment handling and allowing clinicians to focus more on patient care instead of administrative coordination. When a patient books an appointment at 10 pm, receives a confirmation text within 30 seconds, and is automatically directed to the intake process, your funnel is functioning effectively.
Touchpoint 2 – Digital Intake Delays: Mobile Forms Losing Patients Before Arrival
Friction Point: You give patients a PDF or a mobile-unfriendly web form, forcing them back into paper and inefficiencies despite starting online.
Booking the patient is only half the job. The intake process that follows is where most clinics quietly lose the digital gains they just made. These are not digital intake workflows – they are paper workflows with digital packaging, and patients see through them immediately.
Without mobile optimization, patient information forms go ignored, and patients show up for their appointments without completing anything online. They fill out the forms by hand while sitting at the reception counter. Staff must manually enter the information again. You paid twice for the same information – first for a digital intake system that failed, then for staff time re-entering handwritten forms into your workflow.
Software Fix: Use a mobile-first intake tool – most modern EHRs include one, or you can add standalone options like Phreesia or Clearwave. It must auto-save progress, scan insurance cards via camera, and complete in under three minutes on a phone. Send the intake link by SMS 48 hours before the visit.
 PRO TIP
PRO TIP
Touchpoint 3 – Virtual Waiting Room Disconnects: Digital Patient Experience Clinic Gap
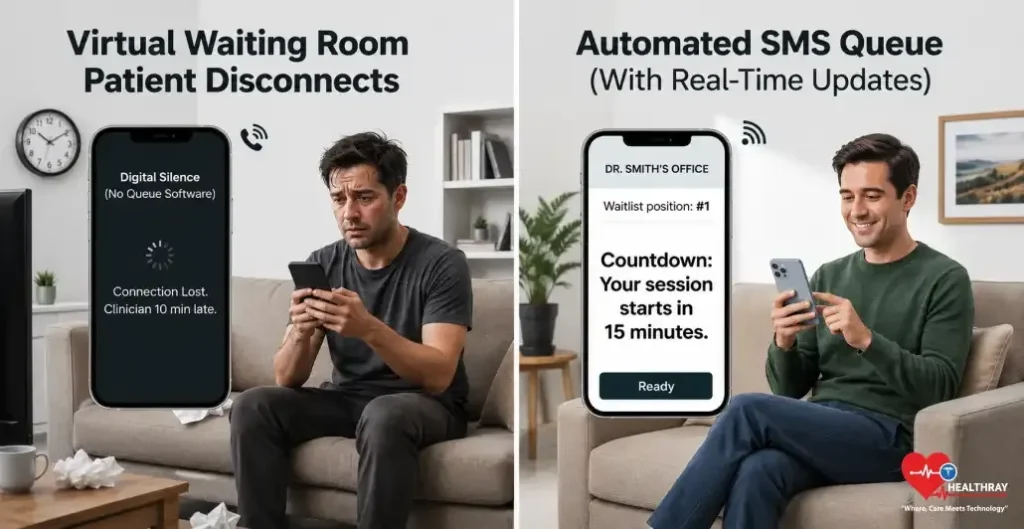
Friction Point: The clinician is 10 minutes behind schedule. No update is sent to the patient. Silence ensues. The patient shuts down the browser. Without timely communication, uncertainty can quickly turn into disengagement. Evidence reviewed through the National Library of Medicine shows that mobile messaging interventions improve patient adherence and attendance, highlighting the importance of keeping patients informed throughout the care process.
Telehealth greatly expanded the capacity of the outpatient clinic. However, telehealth created a new mode of failure that many operations teams have yet to tackle: the waiting room without any kind of communications backbone to support it. A clinician runs behind schedule – which is not exceptional, it is Tuesday – but the patient in the virtual waiting room gets nothing.
After five minutes of silence, there are only two possible conclusions that the patient can make: the system is broken, or the clinic forgot about them. In either case, their actions will be identical – they’ll either call the clinic or log off. The efficiency gain telehealth was supposed to create disappears instantly. When supported by staff scheduling software for clinics, delays can be proactively managed by dynamically adjusting availability and workload distribution, reducing the likelihood of silent wait times. The table below depicts how automated SMS queue management works for each scenario:
| SCENARIO | WITHOUT QUEUE SOFTWARE | WITH AUTOMATED SMS QUEUE |
| Delay | Patient calls front desk | Countdown update sent automatically |
| Dropout | Patient abandons | Re-entry link delivered with one tap |
| Overlap | Staff calls each patient | Notifications sent automatically |
| Follow-up | Patient waits for email | Summary link arrives within minutes |
Software Fix: Develop two-way SMS queue text software that provides dynamic countdown timers and browser executable room links without requiring assistance from any staff. There should be no question left in the mind of the patient about whether anything is happening.
Touchpoint 4 – Billing Friction At Point Of Care: Paper Statements Reducing Collections
Friction Point: A paper statement arrives three weeks after the visit, or a staff member asks a patient to read their card number aloud on the phone. By the time the bill arrives, the visit is a distant memory.
The medical experience was superb. But then, the bill destroys it all. A mailed-out bill almost a month down the line seems impersonal, too late, and easy to forget about, especially if it doesn’t exceed fifty dollars. The patients either deny owing that sum or ignore it. Small debts add up to bad debts.
The data on this is unambiguous. 71% of providers report that it takes over 30 days to collect payments after a patient encounter – switching to digital collection at the point of care changes that equation immediately. However, making the switch to an electronic method such as the text-to-pay system makes it possible to eliminate any form of collection issues within weeks, improving the speed of payment from weeks to days.
Software Fix: Install a merchant embedded text-to-pay functionality along with digital wallet integration right in the checkout process so that payment can be the logical end of the visit, rather than a separate billing cycle that starts weeks down the road. In a digital patient experience clinic, the ability to secure card-on-file information during this point removes the need for collection at all for a portion of the patients seen.
 NOTE
NOTE
Touchpoint 5 – Post-Visit Follow-Up Failures: Where Patient Retention Finally Breaks
Friction Point: Patients go home with their discharge paperwork written out by hand on a printed form. They put it in their bag, then leave it in their car, and never see it again. Lack of digital access causes follow-up failure.
This last point of contact is the most ignored and potentially the most critical for getting patients to return. Discharging patients with paper information makes the process come full circle on paper rather than in your practice management software. These notes are separate from appointment reminders or your patient portal. If patients misplace the paper, as often happens, they can no longer refer to it.
Patient retention can take place here, or not. According to the results of a systematic review carried out by the CDC, a scheduled outpatient follow-up visit could reduce 30-day all-cause readmissions by 21%, provided that patients followed their discharge instructions. However, it will do nothing for patients whose notes are in their cars, never to be seen again.
Software Fix: Set up an automated process to send an SMS and email after the encounter, with links to a secure portal where patients can access their digital care summary within minutes. These systems function as part of modern clinic patient engagement tools, helping maintain communication after the visit and increasing the likelihood of follow-up adherence and retention. Deliver the care summary within 15 minutes of patient departure. Include an option to book the next appointment. This completes the digital patient experience clinic loop, from the first booking to the next visit.
Learn more: Top 10 Clinic Management Software in India (2026 Comparison) for a detailed comparison of tools that improve clinic operations and patient experience.
To Sum Up: Fixing All Patient Experience Touchpoints Across The Journey

Digital friction – not poor clinical care – is why patients don’t return, payments arrive late, and front desks stay overwhelmed. Five touchpoints. Five fixable gaps. And every one of them is recoverable with the right infrastructure layer already available to your clinic today.
The scheduling API ensures your calendar is populated without needing callbacks. Intake processes designed specifically for mobile means no clipboard data entry on appointment day. Automated SMS queues keep patients informed and reduce front desk workload. Text-to-pay at service point improves revenue cycle and reduces collection delays. Digital discharge documents improve engagement and retention more than paper methods. CDC research shows follow-up care can reduce readmissions by up to 21%.
Nothing here requires starting from scratch. It requires connecting infrastructure at five key operational checkpoints in a digital patient experience clinic environment. Clinics using digital patient experience systems report fewer no-shows, faster payments, lower admin work, and higher returns.
The real issue isn’t whether your clinic needs an improved digital patient experience framework. It’s how many patients will cost you before you even fill your next appointment slot.