






































In This Article:
A detailed explanation on the importance of an appointment system integrated with EMR.
- How isolated systems lead to work interruptions, waiting times, and staff exhaustion
- How integration links scheduling information with up-to-date medical data
- How patient identification synchronization, encounter initiation, and information flow help operations
- How timely availability updates eliminate clashes in scheduling and double bookings
- The healthcare delivery decisions being a combination of automated systems and human interventions
- How doing things together in one system enhances work flow, productivity, and health services
The Technical Anatomy of the Integration Layer
A doctor appointment system should do more than just book visits. It should act as a simple, direct part of the patient’s medical record. In busy Indian hospitals, when scheduling and medical records are separate, staff end up overworked, and the chances of errors and fatigue go up.
In order to appreciate how an appointment system with EMR integration functions, it is important to explore the underlying technical protocols that allow two disparate software entities to ‘communicate’ the same language. Given the emergence of the National Digital Health Mission (NDHM) in the Indian healthcare landscape as the standard data-sharing framework, this integration predominantly leverages APIs (Application Programming Interfaces) or HL7/FHIR standards.
The “Single Source of Truth” Strategy
The main objective of integration is to ensure that the EMR is always treated as the “Master” database for all clinical information and that the appointment system acts as the “Active Agent” responsible for acquiring and disseminating the relevant data.
- The Handshake: When the patient inputs their information into the appointment booking portal, the system generates a request to the EMR database to look for a matching UHID.
- The Validation: If a match is found, the appointment automatically gets associated with the medical history of the patient; otherwise, it receives a “Provisional Record” and is validated at the reception upon arrival.
- The Result: This technical integration is such that when a doctor opens the day’s appointment diary, it contains a comprehensive list of clinical profiles and not just a list of patient names.
Real-Time Slot Telemetry
The most common point of operational failure in hospitals is the “Scheduling Lag,” which occurs when a doctor’s schedule gets altered in the EMR (due to a ward round or surgery), while the appointment system still shows them as available.
- The Logic: “Live Telemetry” is a mechanism used by highly integrated systems, whereby any change in the EMR’s clinical calendar gets automatically reflected in the public-facing doctor appointment system in real-time.
- The Benefit: This eliminates the problem of “Double-Booking,” which is so common in the Indian context in high-volume Outpatient Departments, and helps maintain the integrity of the doctor’s schedule and the hospital’s reputation.
 NOTE
NOTE
Evaluating the Integration Scope: The Rule vs. Reason Matrix
Instead of treating integration as an all‑or‑nothing choice, hospitals should review their workflows with a simple matrix. This matrix balances clear system rules with human judgment. This allows them to identify specific data links that must be automated and those that merely need to be ‘suggested’ by the software.
- Logic-Driven Determinism (The Rules)
This segment describes processes based on a clear mathematical or binary logic. For instance, if a doctor’s shift ends at 4:00 PM, no booking can be made for 4:15 PM; these are high-determinism tasks, which do not require human involvement and must be fully synchronized between the recurring doctor appointment scheduling and the EMR, to minimize mental effort on part of the receptionists.
- Clinical Intuition (The Reason)
Healthcare can be mystifying. When a person with long-term high blood pressure has an appointment for a routine “General Check-up” and wonders if they really need a “Cardiac Evaluation,” what would that patient hear if they asked their question? You can set alerts, but you cannot have the system make the proactive calls. In these situations, your instincts come before any algorithm.
- The Four Quadrants of Work
| CATEGORY | TASK EXAMPLES | INTEGRATION MODE |
| Strict Rules / Low Risk | Slot availability, SMS reminders, and matching UHIDs | Auto-Pilot: Data flows on its own |
| Strict Rules / High Risk | Scheduling before surgery, strict fasting rules | Guardrail: The system blocks slots until all requirements are met |
| Subjective / Low Risk | Regularly changing plans and wanting certain cabins | Flexible: The system makes suggestions, and the person makes the final decision |
| Subjective / High Risk | Emergency triage and coordination between specialists | Manual Control: People only use the system to log in. |
High-Impact Data Connections: What Moves and How
Integrating a doctor appointment calendar system requires specific data fields to be connected between the two systems. This is what we call the “Workflow Layer” that sets a routine booking apart from a safe consultation.
1. The Encounter Trigger
The check-in process at the reception desk is probably the most critical data trigger in any integrated system
- The Data: The appointment system tells the EMR that [Patient UHID-1234] has arrived for [Appointment ID-5678].
- The Action: The EMR will automatically create a “New Encounter” for the visit. This is the digital “bucket” to hold all the doctor’s notes, prescriptions, and vital signs for that visit.
- The Workflow: This immediately updates the doctor’s screen to say “In Waiting.” No need to call the doctor or to take the paper slip to their cabin.
2. Pre-Visit Triage Data
Some of the best doctor appointment systems allow patients to fill in a quick form about their symptoms when they book an appointment.
- The Data: A patient’s answers, such as “Fever for 3 days” or “Allergic to Penicillin”, get automatically pulled into the “Chief Complaint” or “Allergies” field of the EMR.
- The Action: The doctor can already see this information even before the patient starts talking: The Action. Instead of spending three minutes typing, the doctor can start the dialogue with “I see you’ve had a fever for three days; let’s look at that.”
 PRO TIP
PRO TIP
Before vs. After: The Impact of a Unified Workflow Layer
If we really want to appreciate the value of an appointment system integrated with the EMR, we have to think about the “Friction Points” in a traditional hospital setting compared to a modern, integrated approach.
| WORKFLOW STEP | THE MANUAL/SILOED WAY | THE INTEGRATED/UNIFIED WAY |
| Vital Signs | Nurse writes vitals on paper; doctor re-types them. | Nurse enters vitals into EMR; they appear in the doctor’s view instantly. |
| Wait Time | “Blind Waiting” for patients; high frustration. | “Live Status” updates sent to patients’ phones via WhatsApp or SMS. |
| The Consultation | Doctor spends 40% of time searching for old reports. | Reports are auto-attached to the current appointment encounter. |
Learn more: Even the best integrated systems fail without proper implementation planning. A Realistic Implementation Steps of Doctor Appointment System for Hospitals shows how hospitals can set up scheduling workflows, staff adoption, and system coordination successfully.
Over-Automation: The Hidden Risk in Indian Healthcare
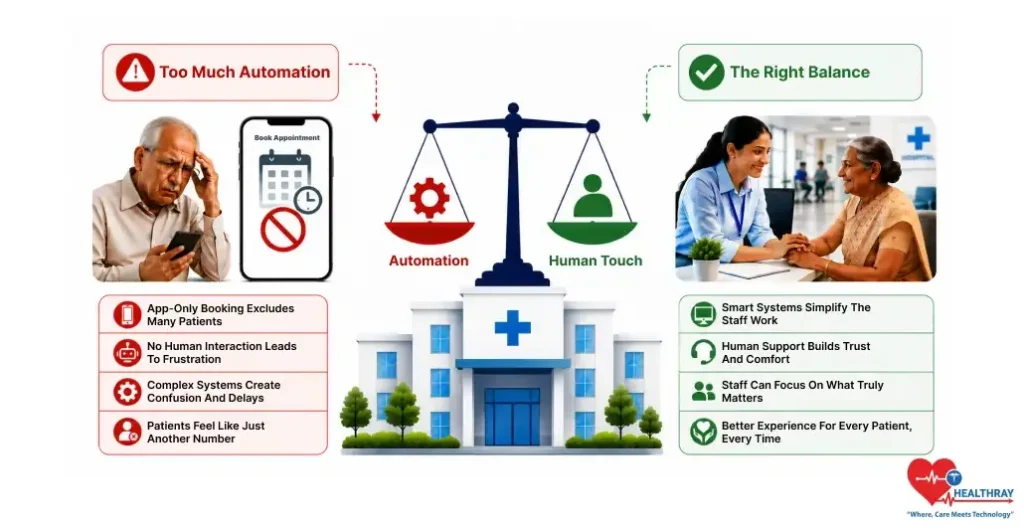
One the greatest threats to Indian hospitals is the “Digital Wall” that can make patients feel like they are no longer talking to people. You over-automate your doctor appointment system for hospitals at the risk of turning off older patients and those who aren’t as tech-savvy.
The risk is creating a system that only takes bookings through an app, which can exclude a substantial portion of your patients who prefer human contact. Instead of automating the doctor’s appointment system for patients, the integration layer should automate and simplify work for your staff.
When your receptionist isn’t spending 10 minutes typing out a patient’s name, they can use that time to walk an elderly patient around the hospital. The “Human Layer” is not a flaw in a system; it is a measure of cultural competency. The “Calculations” get handled by automation and the “Complications” get handled by Humans. As soon as you find that balance, your clinic scheduling software can be a pathway to growth, not a barrier to access.
Conclusion
Having an appointment system with EMR integration is becoming the norm rather than the exception, leading the way to not considering healthcare technology as a collection of tools, but rather a technology ecosystem. With intelligent emphasis on key data links, including bi-directional slot syncing, automated encounter creation, etc., hospitals can automate their workflows while ensuring that the level of human care they desire is still provided.
In a nation where doctors remain stretched thin, automation brings the speed and precision needed to manage large numbers of patients, with the “human-in-the-loop” as the ultimate guardian of clinical intuition and empathy. In the final analysis, a tightly integrated system enables medical staff to devote less time to handling the data and more time handling the patient, and that translates to an overall more efficient, safe and humane system of health care delivery.




