In This Blog
One patient record. Four data exchanges. One process moving through every key system in your healthcare facility – registration, EMR, laboratory, and pharmacy. Below are the exact issues addressed in this process:
- The movement of a single patient record through registration, EMR, laboratory, and pharmacy
- The standard tied to each data field during each exchange
- Where breakdowns in the process usually occur and the data field involved
- Global vocabulary standards that help prevent the breakdowns before they reach the patient
- Why unaddressed data field map gaps may quietly bleed your revenue cycle
Research suggests that duplication of patient records occurs in 8 to 12% of all patient records globally – and in virtually all cases, duplicates can be attributed to one error in one field during the time of registration. The one field will go on and influence everything else: the lab order points to the wrong file, the critical test results notify the wrong doctor, the medication request is sent to the wrong desk for fulfillment. Clinic system interoperability is the one process that prevents this chain of errors. Modern clinic management software ensures that each field gets passed along correctly named, validated, and action-ready throughout every step of the patient journey. This document follows one patient’s record through four real-life scenarios and identifies which fields match what standard where.
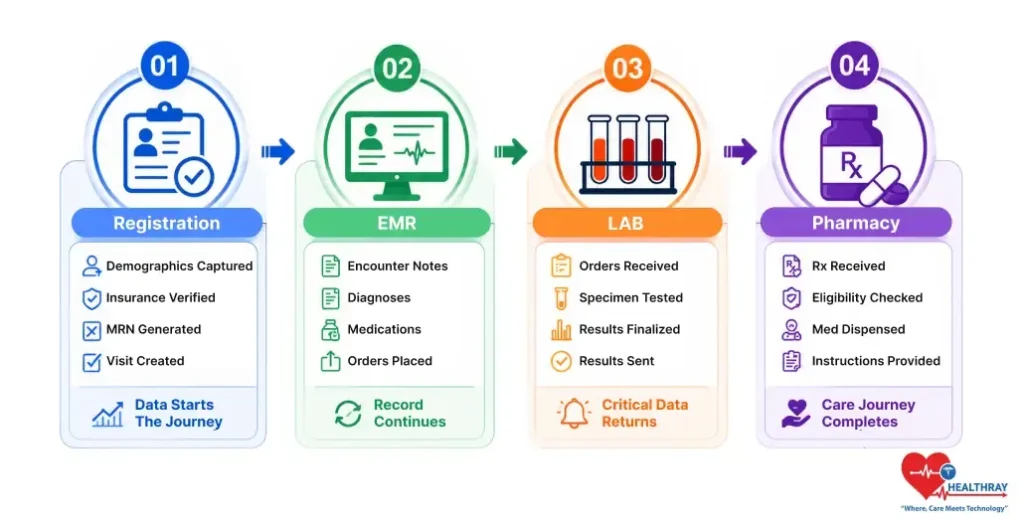
Step 1 – Registration: The Identity Your Data Journey Depends On
Treat registration as the bedrock of clinic system interoperability. The data entered during registration flows across every connected system. When a patient arrives at the clinic, three demographic data points begin the patient data journey.
- Patient Name: Entered into multiple fields within the EMR. A small error, such as placing an initial in the wrong position or incorrectly typing a hyphenated surname, may create a duplicate record because the data no longer matches.
- Date Of Birth: The system uses a standard date format recognized by all systems. If it interprets a country’s format, such as DD/MM/YY, differently as MM/DD/YY, it may create duplicate records for the same individual.
- Patient Sex: The system codes this field using standardized values rather than written descriptions. Search algorithms may treat “M,” “Male,” and “male” as separate entries, while standardized codes remain consistent across systems.
The matching engine of the EMR matches the entered demographic data with existing information on record. The ONC’s Patient Identity and Patient Record Matching guidelines state that matches should be created by at least connecting name, birth date, phone number, and address data. Missing an area code may cause the system to create a new chart.
In multi-location clinic networks, errors can spread across sites. A single incorrectly formatted field may cause duplicate charts across all locations sharing the same patient index. Standardized demographic entry is essential for clinic system interoperability, especially in an automated reminders clinic setting where follow-ups and alerts depend on accurate records. This validated data then accompanies the record to the lab order.
 NOTE
NOTE
Step 2 – EMR To Lab: Where A Signed Order Can Still Disappear
Signature by the doctor on the lab order constitutes a key moment that tests clinic system interoperability, as the EMR verifies and sends the order to the Lab Information System. It is the identity of the patient from step one that forms the order’s base, which is why an issue in any record before then can result in a wrong chart entry or no entry at all. Three things accompany each order:
- Order Tracking Number: The system uses this unique number to identify the order and helps the laboratory match results to the correct patient and encounter. If the system loses or corrupts it during transfer, it cannot determine the destination of the results.
- Test Type Data Standard: Tests should use universal codes rather than local ones. The global standard is LOINC (Logical Observation Identifiers Names and Codes), where each code has the same meaning across all systems, including clinics and reference labs. Local codes only work within the system that created them.
- Ordering Provider’s Identity: Travels as a uniquely identifiable national number, such as a ten-digit NPI in the US or the corresponding clinician identifier in other countries. This ensures consistent provider attribution across all connected systems.
Most interoperability failures occur when non-standard order codes are sent to the lab, causing silent rejections without error messages from the transmitting system. When this happens in a multi-site network, all locations are affected, and it can also disrupt clinic billing software by creating mismatched or unbillable encounters. Once the order is received and accepted by the laboratory, the reverse process begins.
 PRO TIP
PRO TIP
Step 3 – Lab To EMR: The Critical Value That Goes Missing
Once the analyzer processes a sample, the system sends structured results to the EMR flowsheet, converting raw output into searchable data that supports clinical decisions and triggers critical alerts. Clinicians treat errors at this stage as clinical, not just functional. The Step 2 tracking number allows the system to match the result to the correct encounter, but if the number is lost, the system may misfile the result without warning. Each result contains three key details:
- Test Result Value: A numeric value, such as a glucose level of 105, can be recognized and used by EMR systems for automated functions. However, if recorded in narrative text, the system cannot detect or process the number.
- Units Of Measurement: This must be presented in a standardized format using the international system known as UCUM. Different labs may use different text labels to describe their units, but this will render the units unusable for most automatic functions.
- Result Interpretation Flag: Is a flagged indicator that indicates whether the result is within normal ranges, high, low, or critically abnormal. The flag is the element that triggers the alert. If it is unmapped from the lab system to the EMR, it vanishes completely without trace.
A lack of mapping for interpretation flags can result in critically high EMR values without triggering alerts. In multi-site networks, this risk appears across all lab interfaces and may not be detected in every location. Tracking results ensures a proper audit trail for data receipt, mapping, and routing. In a telehealth-enabled clinic software environment, this becomes even more critical as clinicians rely on remote access to lab results for timely decisions. Once validated, the result and encounter move to the pharmacy.
Step 4 – EMR To Pharmacy: One Unstructured Field Holds Up The Fill
The prescribing provider signs the script, and for this last step in achieving clinic system interoperability between clinic systems, it’s critical that the transaction reaches the pharmacy as a structured, unambiguous record. Faxing, scanning, or embedding instructions in a notes field would all introduce some element of human intervention, which becomes a delay factor. There are three key data items that come through on every prescription:
- Medication Identity: Prescribers must use the recognized drug code, not just text. The system applies the RxNorm standard, which assigns a unique identifier to each medication, including its form and strength. For example, without RxNorm, “metformin 500” could be interpreted differently by different pharmacies.
- Dosage Instructions: The system should format prescriptions so computers can read them. If they arrive as text, such as “one tablet per day with dinner,” the pharmacy system cannot process them until a pharmacist reviews them.
- Number Of Refills: Should be a number, not written out. The number 3, not “three.” Any text format entered into a numeric field will prevent automation.
Narrative-based prescribing holds prescriptions pending pharmacy intervention. In a pharmaceutical chain with multiple stores, narrative-based prescribing holds can be repeated daily within each and every store. It is said that “structured data is required for prescriptions,” according to the “Draft Federal FHIR Action Plan for 2024,”
The Complete Data Journey Map: Every Handoff, Every Risk
For a clear understanding of the vital handoff processes in your clinical network, it is useful to get an overview of the movement of data throughout all systems. This table gives an overview of how clinic system interoperability depends on proper field mapping at each process, its governing standard, and the major risk associated with failure.
| HANDOFF | WHAT TRAVELS | STANDARD | FAILURE RISK |
| Registration → EMR | Name, birth date, sex | Normalization | Duplicate charts |
| EMR → Lab | Order ID, test type, provider | LOINC | Orphaned orders |
| Lab → EMR | Result value, unit, flag | UCUM | Alert failures |
| EMR → Pharmacy | Drug code, dosage, refills | RxNorm | Dispense holds |
If you do not resolve any of the fields on this map, the system could quietly ignore or misplace them. Within the realm of healthcare, either situation can have dire ramifications from both an ethical and financial standpoint.
The Bottom Line: What These Handoffs Are Really Costing You
You have now followed the journey of a single patient file through four different systems: registration, EMR, laboratory, and pharmacy – a complete example of clinic system interoperability. At each step of the way, the slightest problem with formatting and mapping could disrupt the process: a duplicate file, a lost order, a missed alert, or even a pending prescription.
This problem is not just theoretical. Duplicate data leads to denied claims. Failed lab orders lead to billable interactions that cannot be recovered. Time spent on managing pharmacy holds takes away from other work. Failure to act on a critical alert exposes the clinic to unnecessary risk.
The best clinics at data quality do not necessarily use the most advanced technology. These are the clinics that fill all their gaps, be they in registration, lab orders, results, or prescriptions, and document it through an audit trail. Every single gap outlined here is already present somewhere within your network. The real question is not about presence but about pinpointing its exact location.
Learn more: Role-Based Access in Clinic Software: Who Sees What Data, showing how access controls intersect with interoperability to keep sensitive data secure and actionable.