






































In This Blog
Hospital requirements to consider before implementing an online doctor appointment management system:
- Why most hospital scheduling systems fail after implementation
- How unauthorized shadow bookings create significant operational confusion
- The critical importance of proper HIS/EMR system integration
- Why effective staff training is more important than software features
- How thorough stress testing prevents OPD scheduling failures
- Hospitals’ essential requirements after a successful system rollout
Strategic Deployment – Mapping The Operational Transition
One can imagine the process of implementing this change as changing the engine of a machine that is fully working in the hospital. There is no way to stop the process or to wait. Consultations must continue, emergencies can occur at any moment, and front-desk staff already handle heavy workloads without additional screens.
The main purpose of our strategy should be to shift away from manual scheduling practices such as personal notebooks, WhatsApp communication between coordinators, and other informal methods. The goal is to move toward a data-based scheduling approach where outcomes remain consistent regardless of who is managing the process. This also allows hospitals to better evaluate and implement a doctor appointment system that supports this transition.
However, this process starts to fail at its very beginning when the software logic is created based on assumptions and does not take into account real-life situations.
Phase 1 – The Audit Of Chaos And Shadow Systems
Before implementing the software configuration, the team must analyze how the hospital actually manages bookings in practice, not just how they appear on paper.
In most cases, there is a huge difference between the two approaches. For example, one system shows rooms as vacant, while another blocks them for weekly department meetings. Similarly, consultants schedule 30-minute slots but consistently take at least 45 minutes per appointment. A front desk coordinator used to organize all the bookings via WhatsApp chats for the last 5 years and will continue to do so unless anything else is offered.
Those are shadow systems. They are present in every hospital, and there is no inherent problem in them because they represent a natural reaction to a system that failed to match clinical reality. But the problem arises when you try to introduce a doctor appointment calendar system into your hospital on top of shadow systems without understanding and reorganizing them.
Deliverables from Phase 1: A complete chart of non-official booking methods, a standard rules book for availability of rooms, and a classification of appointment types, along with allocated time durations such as a follow-up of 15 minutes as compared to an initial consultation of 45 minutes.
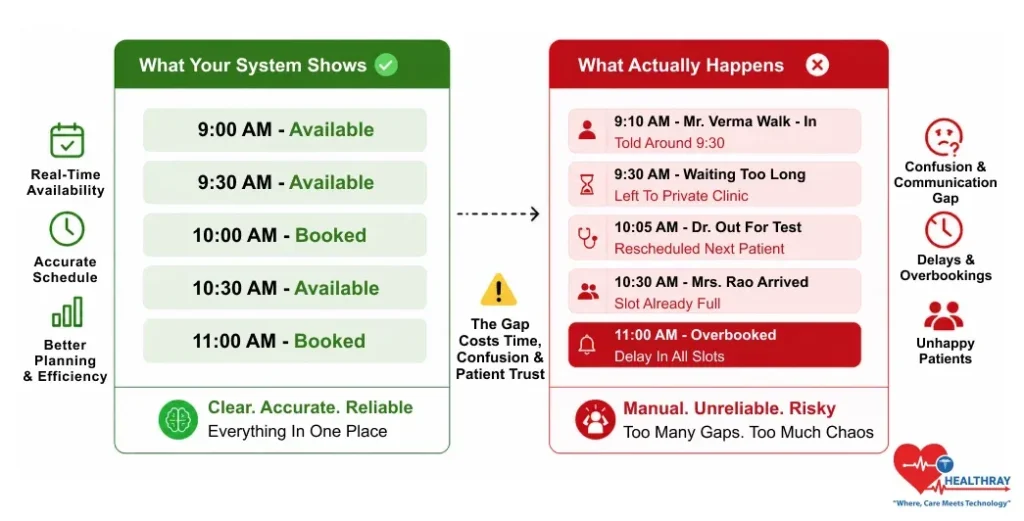
In a hospital located in Pune, the scheduling process displayed availability until late morning hours, although in practice the waiting area was packed because of bookings through telephonic contacts, direct visits, and manually made arrangements that did not make it to the computerized records.
Phase 2 – The Integration Layer And Technical Sync
The issue of technical integration is where many promising systems fail to materialize, especially after hospitals realize that recurring doctor appointment scheduling must align with real-world clinical workflows. This appointment system must be able to talk clearly to the hospital’s existing HIS and EMR system. Otherwise, the system will work in isolation, scheduling appointments without taking into account the patient’s medical history.
The standard that provides guidance on how scheduling information such as slot availability, patient identification, and physician assignments must be formatted and transmitted is the HL7 FHIR Appointment Resource standard. Systems that ignore this standard will be prone to instability, difficult to maintain, and almost impossible to audit.
 NOTE
NOTE
The second significant risk in this phase is data migration. Typically, most hospitals maintain large datasets filled with uncleaned data. There are duplicate patient records, varying naming conventions, and some data exists within one hospital system and not another. The migration of this data without proper cleansing leads to the creation of ghost patients, which refers to patients that appear in your booking system without having any corresponding medical data records.
Phase 3 – The Human Element And The Training Pivot
It is seldom because of technology that the doctor appointment system for hospitals breaks down. Humans do. More precisely, failure occurs when a frazzled front-desk clerk turns to the old-fashioned paper diary instead of the newly installed software during a busy Monday morning, often due to training gaps despite support from tools like a branded video production company for internal communication.
Training should never be a single-day activity, and many hospitals now use structured video-based learning platforms, including a Uscreen alternative, to make onboarding more consistent and easier to repeat across departments. Make it a behavioral change initiative that goes beyond simply teaching people how to use the software. It should also include an explanation of what problems arise later on as a result of neglecting the software.
 PRO TIP
PRO TIP
From the perspective of the patient, the SMS/WhatsApp reminders sent automatically by hospitals are an improvement – but only if they use the correct timing. Sending too many reminders means patients will end up blocking the sender ID. When an actual emergency arises, they’ll never receive it.
Phase 4 – Stress Testing And The Implementation Risk Matrix
Prior to go-live in any busy OPD, testing should cover loss of connection and simultaneous booking rushes. It should also include late doctors after OT duty and unexpected emergency walk-ins disrupting schedules.
Every deployment requires a no-fail manual backup procedure. Everyone should know how to deal with a situation where the cloud is down. Hospitals that neglect this will face failure on day one, in front of a full waiting room.
Buffer management is the most underappreciated function in any scheduling software. Creating empty time slots in between ensures one missed appointment doesn’t ruin the whole afternoon schedule.
Implementation Risk Matrix for a Comprehensive Doctor Appointment System for Hospitals
| PHASE | OPERATIONAL RISK | BREAK POINT | MITIGATION STRATEGY |
| Audit | Tribal knowledge | Shadow system | Unofficial slot booking documentation |
| Integration | Data silo | Ghost account | HL7/FHIR standard compliance |
| Training | Staff resistance | Bypassing system | Conflict management training |
| Go-Live | Domino effect | Lobby collapse | Weighted slots & buffer gaps |
Learn more: Best Doctor Appointment Systems Compared with Real Market Data breaks down how modern scheduling platforms handle buffers, physician load balancing, and operational scalability in real hospital environments.
Phase 5 – Post-Implementation And The Fix-It Phase
Go-live is not the end goal. It’s merely the trigger for an entirely new type of task: Observation, gap analysis, and iteration. But the key change to make after go-live is shifting the paradigm from project to product.
One of the earliest comparisons to conduct will be between scheduled time and actual observed time. When the schedule indicates 15 minutes for follow-ups, but each actually lasts 25 minutes, the slot length is incorrect. As a result, all scheduling calculations are based on faulty assumptions, which is why many hospitals rely on medical scheduling tools to continuously measure and optimize real appointment durations.
“Ghost appointments” – bookings created by administrative errors – increase no-shows and distort performance metrics. Hospitals usually implement detection logic post go-live, often after performance data is already corrupted. Based on an ONC data brief about interoperability in US hospitals, the use of physician data increased from 26 percent to 70 percent where hospitals ensured their digital infrastructure was always up-to-date. An advanced appointment scheduling system in hospitals will never be complete.
To Sum Up: Why Hospital Scheduling Cannot Be Rushed
The scheduling system of appointments in hospitals will only work if the hospital makes its preparations well before relying on technology to solve the problem. The doctors are always late. There are walk-ins. The staff falls back into their old ways because of the pressure. The patients fail to heed the reminders. This is reality in operations, and good implementation should consider it when deploying a doctor appointment system for hospitals.
Those hospitals which keep improving their scheduling process, track actual appointment times, and continue training after go-live are the ones that really alleviate waiting room stress and increase efficiency.
As far as hospital scheduling is concerned, success is not reached during implementation; it is reached only after go-live.




